© 2026 Blaze Media LLC. All rights reserved.
“Speak no ill of Medicaid” appears to be the guiding principle of those seeking to identify and solve the drug overdose crisis.
The only way to explain the timing of the precipitous epidemic of the 400-600 percent increase in overdoses in the years 2013-2016 is to understand the amalgamation of the border surge and Medicaid expansion happening around the same time.
In our series of articles on the drug overdose crisis, we have demonstrated that what the political class refers to as an “opioid crisis” and claims to be solving by addressing prescription overdoses – is in fact a fentanyl and heroin crisis fueled by a massive influx of drugs due to immigration and border policies.l
Say it with me: It’s not prescriptions
Incontrovertible data show that prescriptions for opioids are plummeting because of the new restrictions put into place, for better or for worse, yet deaths from heroin and fentanyl are surging. The rate of high-dosage prescription opioids has been nearly cut in half, yet the rate of fatalities has dropped only slightly in many states. As such, more of a focus on restricting prescriptions without dealing with the supply of heroin and fentanyl will be counterintuitive and allow even more fatalities.
The next logical question is this: If supply of prescription drugs is so tight, and in turn, prescription drug overdoses are going down while illicit drug overdoses are skyrocketing, do we have a prescription overdose problem at all? The answer is that while prescription deaths have gone down in most states, they have not dropped nearly as much as one would expect, given that prescriptions themselves have plummeted. Accordingly, many patients who need painkillers and are not addicts are having trouble getting them, but at the same time, a number of Medicaid patients have access to dirt-cheap prescriptions.
What was the 800-pound gorilla in the room that changed the health care landscape in around the same time the drug crisis began? Look no further than the Medicaid expansion of Obamacare.
According to a report by Sam Adolphsen of the Foundation for Government Accountability presented as testimony before the Senate Committee on Homeland Security and Government Affairs earlier this year, 13 of the 15 states with the highest opioid overdose rates are Medicaid expansion states. And they account for all five of the top five overdose states. Throwing tens of millions of able-bodied adults on a program that offers very poor access to quality long-term care but offers drugs for absolutely free will takes its toll on market forces and personal incentives – with deadly consequences.
Six data points that demonstrate Medicaid is a culprit
Let’s remember, when it comes to health care, unlike most other industries, the individual consumer is not the consumer. Government programs are the consumer and fuel an artificial demand that affects the supply of drugs.
Here are some more staggering observations:
- Medicaid recipients who are also on TANF, which means they have children at home with access to the medicine cabinets, have the highest rate of opioid prescriptions.
- While Medicaid covers an unbelievable 20 percent of the entire population, it accounts for a gargantuan 36.5 percent of opioid overdose patients, particularly 40 percent of those overdosing on heroin and 47 percent of those overdosing on methadone.
- Timing is key. We’ve long had an addiction problem, but the crisis levels only began after Medicaid expansion. In 2011, 120,000 opioid overdose patients in hospitals were on Medicaid. In 2015, that number rose to 280,000. Liberals like to tout Medicaid as a solution to access more drug rehab programs for free, but the sick irony is lost on them that Medicaid is fueling the addiction of their patients to begin with, in the classic cycle of government. Even before the expansion, a 2009 CDC report showed that in Washington state, Medicaid patients were 5.7 times more likely to die of an opioid overdose than others.
- Overdoses from painkillers quadrupled from 1999 to 2013 (while illicit drug overdoses more than quadrupled in just the past few years). Guess what else happened over the same time period? According to a 2016 Health Affairs study, out-of-pocket spending on opioids declined over a similar period of time – from $4.40 to $0.90. Who pays for the rest? Government, most prominently Medicaid. Remember, the number of people on Medicaid more than doubled since 2000, and enrollment has already spiked 23 percent since 2013.
- According to a new report from the Senate Homeland Security and Government Accountability Committee, “Medicaid has contributed to the nation’s opioid epidemic by establishing a series of incentives that make it enormously profitable to abuse and sell dangerous drugs.” The report found, “Drug overdose deaths per one million people are rising nearly twice as fast in expansion states as non-expansion states, while opioid-related hospital stays paid for by Medicaid massively spiked after expansion.” For example, in Clay County, Kentucky, in just three years, the percentage of those on Medicaid spiked from 35 percent to 60 percent. Concurrently, opioid use spiked, and the waiting list for drug facilities rose 50 percent.
- Another study found that almost a quarter of Medicaid members received the same pain medication from different prescribers: 8.9 percent received meds from four or more prescribers! What this tells us is that addicts are using multiple doctors and multiple pharmacies to escape any scrutiny. But this can only be accomplished when every doctor’s visit and drug filing is free. Someone paying for part of each medical service will think twice before running up the tab. Thus, while doctor-shopping across the board is relatively low, as John D. Lilly demonstrated in a PowerPoint presentation, it is most evident among Medicaid patients. Moreover, according to the National Survey and Drug Use and Health, half of the drug abusers received their drugs from friends or relatives. Who has extra painkillers lying around to give out like candy? Only those who get them for free.
How Medicaid fuels a black market of illicit “prescription” drugs
The reality is that a lot of people need the painkillers they are being prescribed. But to the extent that people are overusing them, the lack of financial barriers plays a big role. A person would be more likely to “tough it out” with Advil when he is in borderline need of painkillers and the cost is not dirt cheap. Then, as noted in the FGA testimony, much of the free money access to Medicaid is being used to create an underground black market to barter for both prescription and illicit opioids.
Detective Nick Rogers of the Denver police explained the dynamic as follows at a congressional hearing:
Many of the people we arrest selling pills come straight from the pharmacy. Those individuals have legitimate prescriptions but sell them for profit. In other words, the suspect gets prescribed 120, 20 milligram oxys, pays nothing for the prescription due to being on government assistance, and makes $2400 for the pills.
Which is why most of the deaths even on the prescription side are attributable to the black market, not to the legitimate practice of medicine. The Medicaid population is already more vulnerable to drug abuse in many states. A study from Express Scripts, one of the largest pharmacy benefit management dispensers to Medicaid patients, states that those on Medicaid are 10 times more likely to suffer from addiction and substance abuse. They found that 6 percent of all Medicaid prescriptions filled were for opioids and nearly 1 in 4 Medicaid patients were prescribed at least one opioid. And according to the 2014 National Survey and Drug Use and Health, more than three-fourths of those who abuse pain medication already had used other drugs before. This is why so many of the deaths that are ascribed to “prescription opioids” on toxicology reports are really the result of mixing those drugs with heroin or alcohol and sleeping pills. But now that a subset of largely the same people who already were addicted to illicit drugs get free access to prescription drugs for the inevitable ailments plaguing them as a result of their lifestyle, they are abusing oxycodone pills as they would heroin.
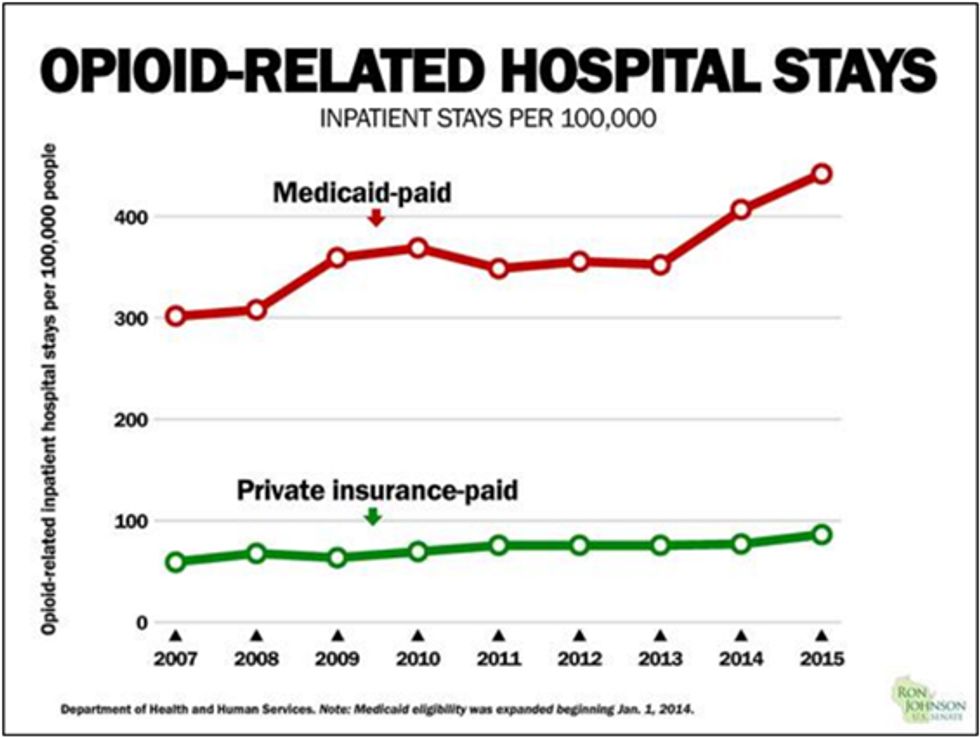
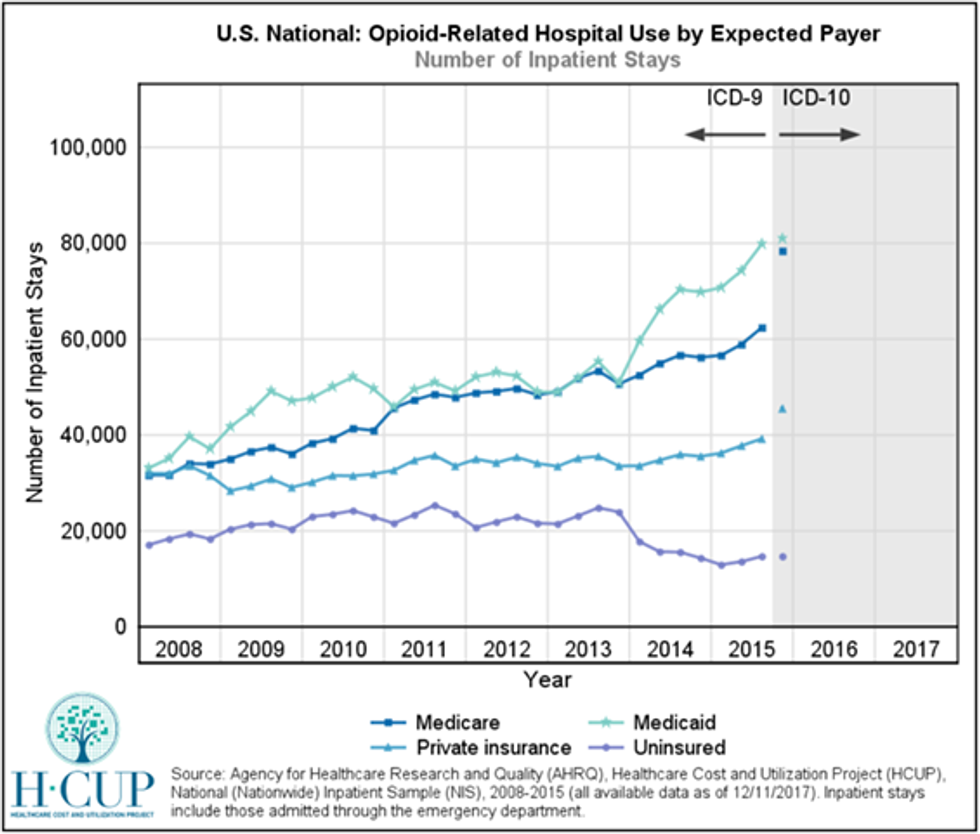
Between 2013 and 2015, ER visits and inpatient stays for overdoses soared among Medicaid patients much more than for those with private insurance, according to the HHS’s Agency for Healthcare Research and Quality.
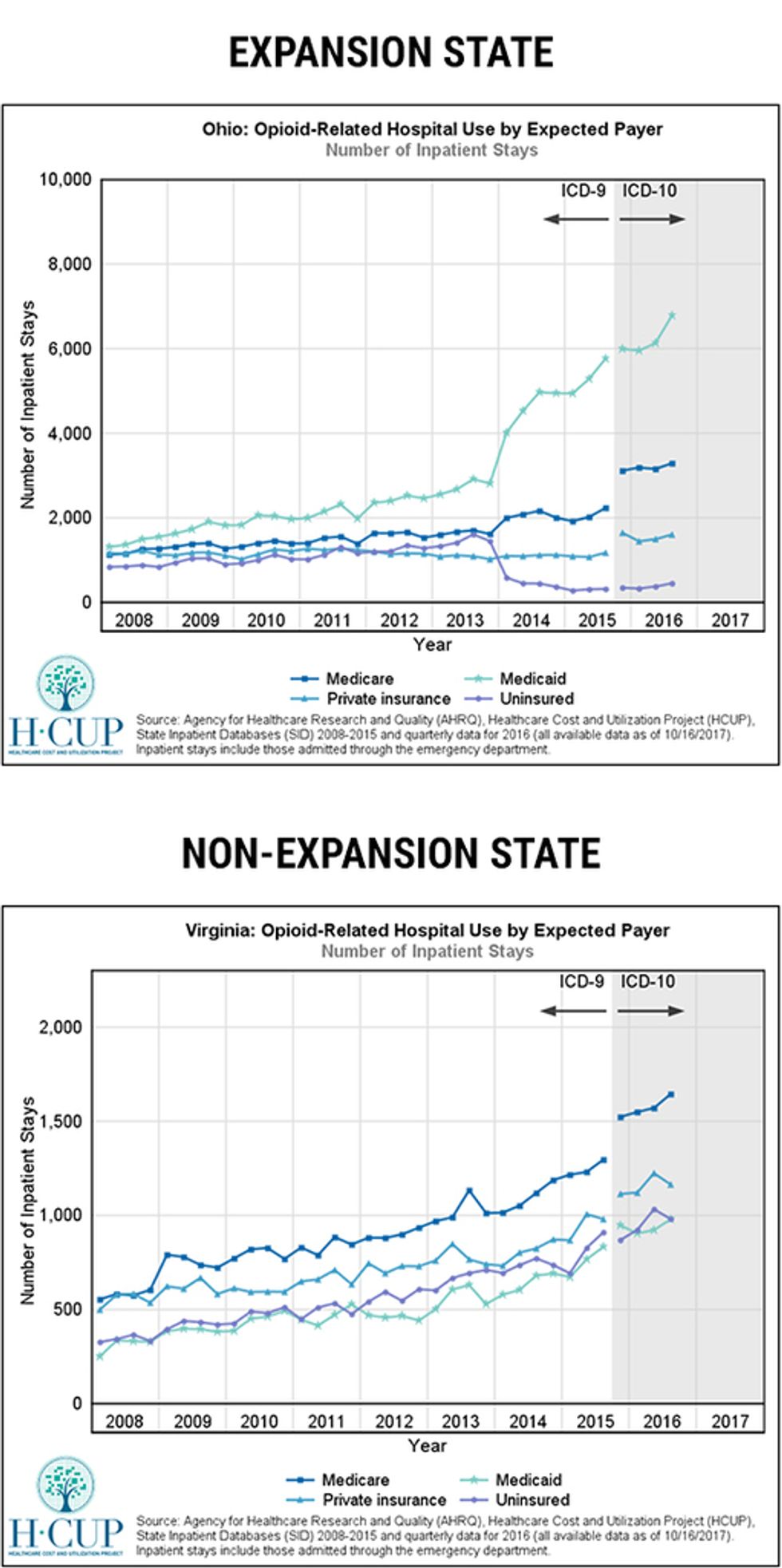
If you play around with the HHS database and sort by Medicaid expansion state vs. non-expansion states, the surge in expansion states around 2013 is remarkable. Look at this comparison between Virginia (non-expansion state) and Ohio (expansion state).
Harking back to our original question: How it is that prescriptions have decreased dramatically to 2002 levels, yet drug deaths are skyrocketing and even prescription deaths are not dropping commensurate with the decreased prescriptions? We now have our answer. Prescriptions are not the gateway to heroin; for the most part, it’s likely the opposite. It’s likely that much of the same population in states like West Virginia that have become hooked on heroin or meth thanks to the open-borders agenda driving up the supply are then taking their addiction to the pharmacy for prescription painkillers as well, thanks to the free Medicaid. According to the West Virginia Department of Health and Human Resources, 71 percent of the 880 people who died last year in West Virginia due to drug overdoses were on Medicaid, even though the majority of the actual deaths for younger users were caused by heroin and fentanyl. Half of them had high to very high Medicaid claims prior to their deaths. And a high percentage of them received pills from three or more prescribers, while those who died were 70 times more likely to have filled prescriptions in four or more pharmacies relative to other drug users monitored by state government. That is a hallmark of the Medicaid-driven doctor-shopping.
In Maine, another overdose hotspot in recent year, a report prepared by the state attorney general showed that most of the cases of death from overdoses of prescription drugs (which trended down in general, not up), the drugs were not prescribed to the decedent. Which means this is either part of the illicit market or was diverted through free government-funded scams, not the result of careless doctors.
The overwhelming evidence of doctor- and pharmacy-shopping from some Medicaid users demonstrates how many who begin with a legitimate prescription then use their past ailment as a means of getting endless taxpayer-subsidized pills for free and then selling them for a profit.
See no evil in Medicaid; restrict and monitor everyone else
Even without the black market, the federal government limits the ability of states to restrict Medicaid coverage of opioids (while encouraging other programs and private insurance to limit coverage). Medicaid is supreme and cannot be touched. Of course, there are many Medicaid patients who are prescribed painkillers and are not drug addicts, and there are those who pay their own way and become addicts, but the numbers don’t lie: Medicaid is a big factor in the problem.
This is how the two policies – open borders and Medicaid – come full-circle. Aside from fueling both over-consumption and fraud through endless taxpayer subsidies, Medicaid patients naturally overlap with the population overdosing on illicit drugs as a result of the cheap influx through the border/immigration policies. Otherwise, why would overdoses still be rising after states have already enacted policies restricting production and prescription of opioids?
#mc_embed_signup{background:#fff; clear:left; font:14px}
/* Add your own MailChimp form style overrides in your site stylesheet or in this style block.
We recommend moving this block and the preceding CSS link to the HEAD of your HTML file. */
Amazingly, the government is stubbornly pursuing policies that restrict coverage for Medicare patients who legitimately need painkillers while ignoring the role Medicaid plays. The background memo for this week’s hearing at the House Energy and Commerce Committee points the finger at Medicare funding, observing that “there is mounting evidence of opioid misuse in the Medicare system.” Yet, when discussing Medicaid, the memo does not mention a word about the free funding of the supply and only touts even more Medicaid spending as the solution to perpetuating addiction treatment programs. Medicaid is simply untouchable.
This is the worst possible policy outcome, because this means that many of the people who legitimately need painkillers will not get them, while Medicaid continues to provide an opportunity to doctor-shop for free.
Rather than set up prescription drug monitoring programs to surveil all doctors and patients, why not end the crony Medicaid expansion for able-bodied adults and convert the program to a defined benefit rather than an open-ended credit card?
Undoubtedly, the addiction crisis in America is due to the amalgamation of multiple complex and seemingly disparate factors that exacerbate the worst elements of one another. Some of the factors are not political at all. But for politicians to ignore the glaring timing of the surge in the crisis and the role open borders and Medicaid played in it – and continue to play – is willful blindness. To downright advocate sanctuary cities, preventing us from decreasing the supply of illicit drugs, and to advocate the continued growth of Medicaid, fueling the demand on both the illicit and prescription sides, is like using a blowtorch instead of a hose to put out a blaze.
As Sam Adolphsen said, “As legislators debate the specifics of repealing and replacing Obamacare, they should resist the feel-good talking point that Medicaid is a silver bullet for solving the opioid epidemic. In reality, Medicaid may be fueling the problem and may be largely responsible for starting the epidemic in the first place.”
Editor's note: A typo in John D. Lilly's name has been corrected. CR apologizes for the error.
Want to leave a tip?
We answer to you. Help keep our content free of advertisers and big tech censorship by leaving a tip today.
Want to join the conversation?
Already a subscriber?