Photo By Tom Williams/CQ-Roll Call, Inc via Getty Images
Editor's note: This story is reposted from Allie Beth Stuckey's website.
*****
Many media outlets are reporting on an increase in cases and pediatric hospitalizations due to COVID. In response, cities, counties and school districts are implementing mask mandates. In some areas, like Dallas County, children as young as 2 years old will be required to wear masks in commercial entities.
To be frank, I find this insane. Considering all the data available that shows the lack of efficacy of most masks in most settings, especially in kids, there is no apparent reason to mandate masks for schools.
Before we get into it, let me say that I have never been an outright anti-masker, and I sure as heck have never believed COVID-19 is some kind of hoax.
I know people whose families have been seriously, negatively impacted by the virus, so I have seen its severity. Also, I'm a germaphobe and a bit of a hypochondriac; it doesn't take much to make me scared of a virus. Back when we thought COVID had a 20% death rate, I was one of the people screaming from the rooftops (aka Twitter) that people need to stay inside. I was sanitizing my groceries, for crying out loud. (I may or may not still be sanitizing my hands every five seconds.)
But, as time went on, and 15 days to slow the spread and relieve the hospitals turned into months of shifting goal posts and mixed messages that seemed to be more correlated with politics and public opinion (here's one example) than science, it became clear that many of our public health experts, and certainly our politicians, really aren't trafficking in fact.
From everything I've read from the world's leading researchers, the science shows there are certain situations in which certain masks worn a certain way by certain people may be effective at preventing the spread of COVID, but even that is debatable. Personally, I think the risks far outweigh the benefits of masking kids. But, I'll present you with the data, and you can decide for yourself.
First, let's talk about this Delta variant that's sent everyone into a tizzy — kind of for good reason, but also kind of not.
The Delta variant is causing a spike in cases, and there is an increase in hospitalizations, too. But we're still nowhere near where we were at our peak in January as far as deaths go. Vaccines could get the credit, and/or it could be that the strain isn't actually as deadly as the original. And, as we'll get to more later, the AAP found that pediatric hospitalization numbers are being inflated because of the CDC's requirement for testing.
Plus, if Delta goes the way it's gone in the other countries it's passed through, it's going to spike then steeply drop off.
Data from India (where Delta originated), Netherlands, and the UK all show a spike in cases due to Delta and a sharp decrease. This data is compiled by the New York Times.
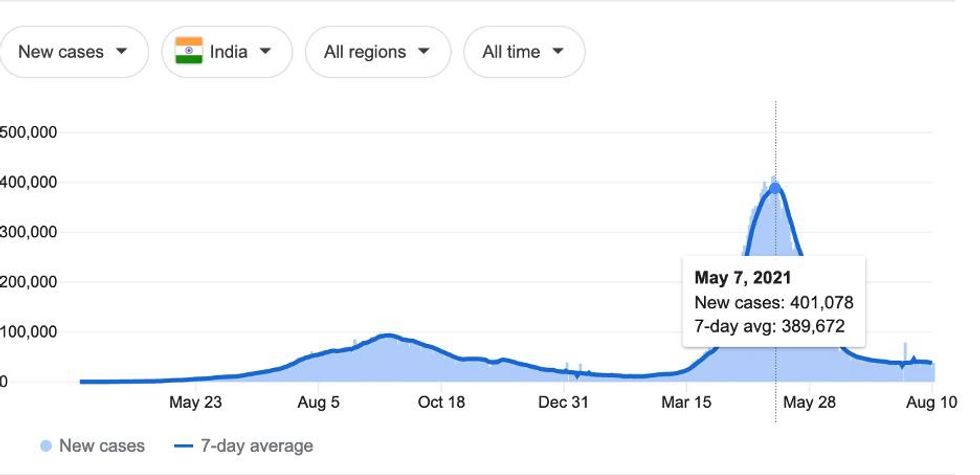
Delta rose and fell in India. Mask compliance remains low in the country (32%).
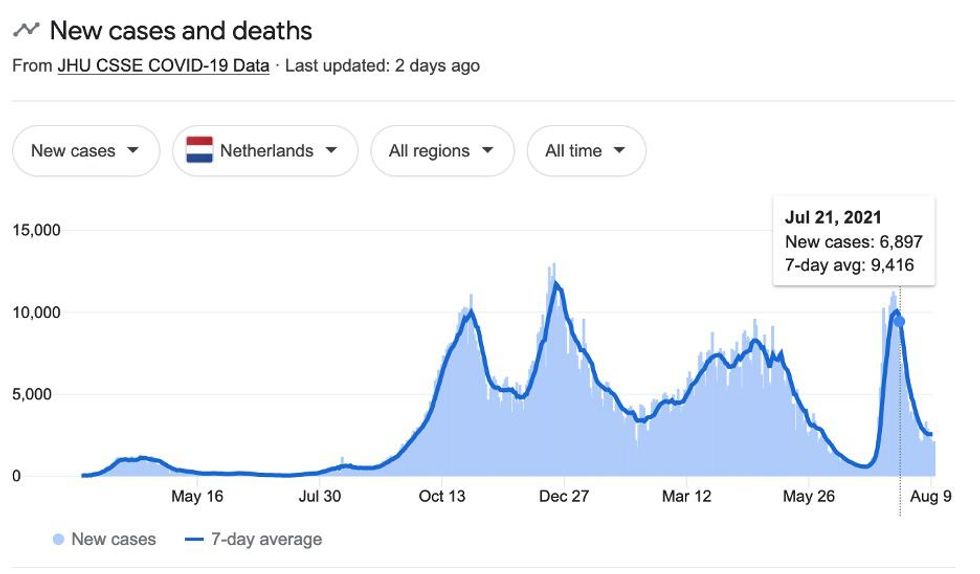
Delta rose and fell in the Netherlands. The country ditched masks in most places on June 26, and they are only required in some spaces for people 13 & over.
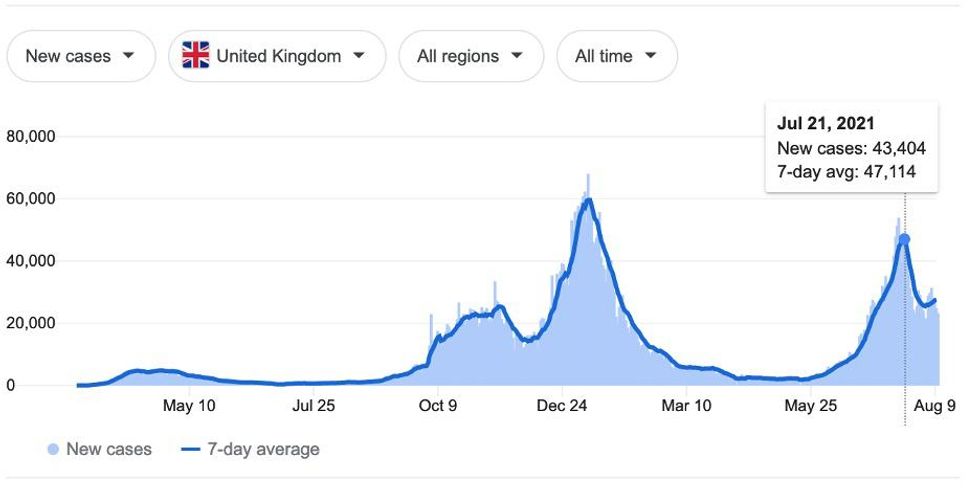
Delta rose and is still falling in the UK. Masks are not required in England, are enforced in some places in England and Wales, and are not required in Northern Ireland for worshipers or students in classrooms.
Delta will do the same in the United States as it has in other countries — spike, then fall — regardless of universal masking.
We really don't have a lot of evidence of mask mandates staving off the virus at all.
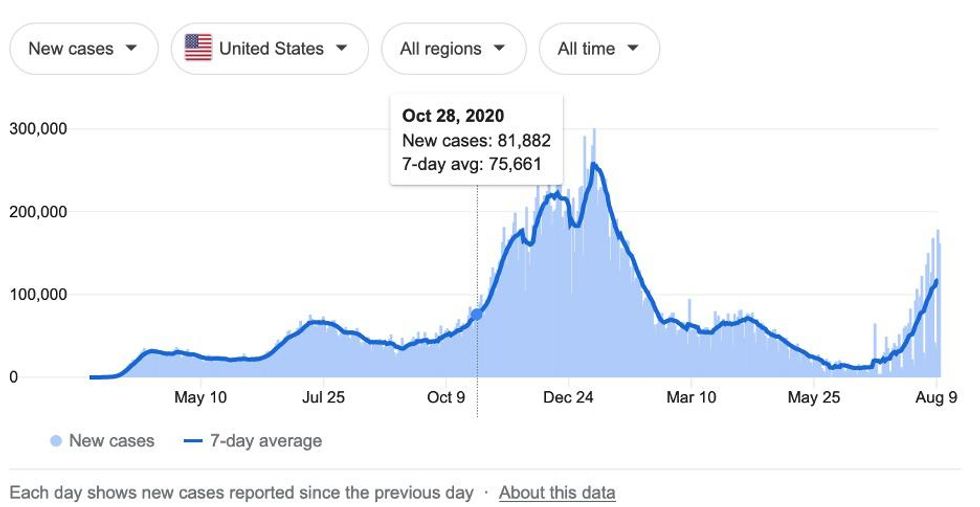
In late October 2020, 93% of adults in the United States reported that they sometimes, often or always wear masks when they leave their home. 72% said they always do. (That puts us right on par with Germany, and ahead of other European countries, as of January 2021.)
And yet data from the NYT shows that the end of October marks the beginning of the biggest spike in COVID cases:
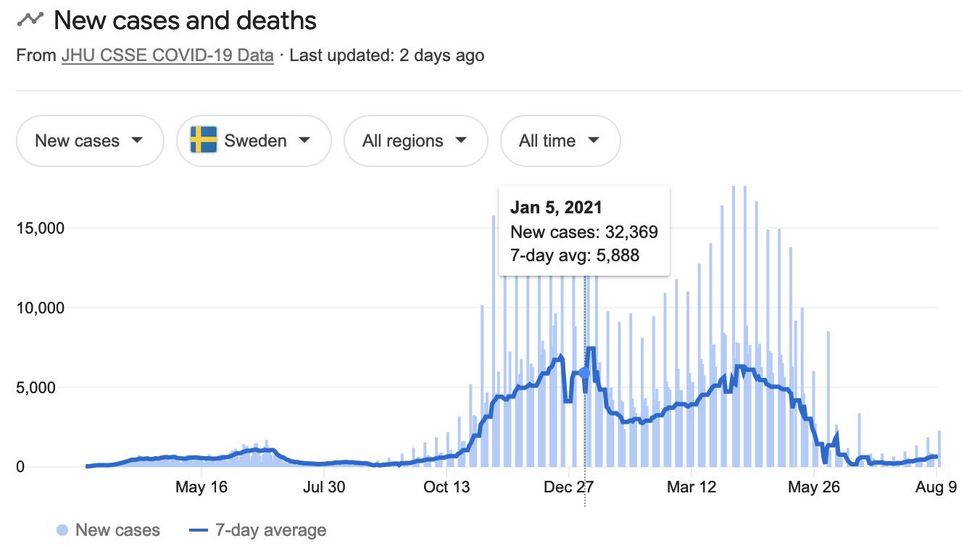
Sweden never mandated masks. In January, only 12% of Swedes said they wore a mask all the time, with 59% saying never. They haven't fared any worse than we have, and their death rate is lower than some other European countries, like those in the UK, who have had mask mandates.
We can also compare Sweden to a U.S. state with a similar population size, Michigan, which implemented its mask mandate in March 2020. While Sweden has had slightly more cases than Michigan (1.11 million vs. 1.02 million), Sweden has had far fewer deaths than Michigan (14,658 vs. 21,243).
Yinon Weiss, a reporter at the Federalist, graphed COVID case stats from Our World in Data of European countries, as well as states in the U.S. and pinpointed when each national and state government implemented mask mandates. What he found was that mask mandates seem to have no effect on the spread of the virus. *See charts toward the end of the article.*
A recent example is Israel, which reinstated its mask mandate on June 25.
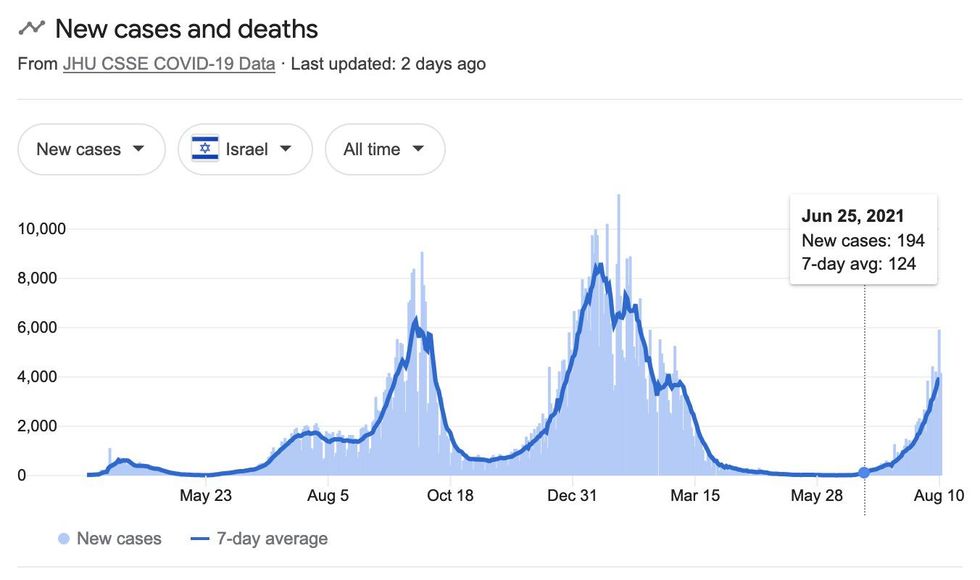
As you can see, Israel's cases have risen in a similar fashion as other countries, like Netherlands, which did the exact opposite — they ditched their mask mandate right before the rise in Delta cases.
Sweden never mandated masks (and has even created a stigma around them) or locked down. Their death rate is much lower than some other European countries that have mandated them, like countries in the UK.
Now, there are other studies looking at other states and countries that do show that cases began to decrease after a mask mandate. But I believe that's more coincidence than causation. Why? Because of the many studies that have already been done on the effectiveness of masks at stopping the transmission of disease.
Mask mandates aren't proven to do much because masks aren't proven to do much.
Several studies demonstrate this:
● The Centre for Evidence-Based Medicine at Oxford University points out that research on the efficacy of masks to prevent the spread of COVID is weak:
In 2010, at the end of the last influenza pandemic, there were six published randomised controlled trials with 4,147 participants focusing on the benefits of different types of masks. Two were done in healthcare workers and four in family or student clusters. The face mask trials for influenza-like illness (ILI) reported poor compliance, rarely reported harms and revealed the pressing need for future trials.
Despite the clear requirement to carry out further large, pragmatic trials a decade later, only six had been published: five in healthcare workers and one in pilgrims. This recent crop of trials added 9,112 participants to the total randomised denominator of 13,259 and showed that masks alone have no significant effect in interrupting the spread of ILI or influenza in the general population, nor in healthcare workers.
It would appear that despite two decades of pandemic preparedness, there is considerable uncertainty as to the value of wearing masks. For instance, high rates of infection with cloth masks could be due to harms caused by cloth masks, or benefits of medical masks. The numerous systematic reviews that have been recently published all include the same evidence base so unsurprisingly broadly reach the same conclusions. However, recent reviews using lower quality evidence found masks to be effective. Whilst also recommending robust randomised trials to inform the evidence for these interventions.
Many countries have gone onto mandate masks for the public in various settings. Several others — Denmark, and Norway — generally do not. Norway's Institute for Public Health reported that if masks did work then any difference in infection rates would be small when infection rates are low: assuming 20% asymptomatics and a risk reduction of 40% for wearing masks, 200 000 people would need to wear one to prevent one new infection per week.
● The New England Journal of Medicine concluded this in May 2020:
We know that wearing a mask outside health care facilities offers little, if any, protection from infection. Public health authorities define a significant exposure to Covid-19 as face-to-face contact within 6 feet with a patient with symptomatic Covid-19 that is sustained for at least a few minutes (and some say more than 10 minutes or even 30 minutes). The chance of catching Covid-19 from a passing interaction in a public space is therefore minimal. In many cases, the desire for widespread masking is a reflexive reaction to anxiety over the pandemic.
● A randomized controlled trial in Japan testing for the effectiveness of surgical masks in reducing the incidence of the common cold found, "Face mask use in health care workers has not been demonstrated to provide benefit in terms of cold symptoms or getting colds. A larger study is needed to definitively establish noninferiority of no mask use."
● A 2010 study by Cambridge University found, "While there is some experimental evidence that masks should be able to reduce infectiousness under controlled conditions, there is less evidence on whether this translates to effectiveness in natural settings. There is little evidence to support the effectiveness of face masks to reduce the risk of infection."
● A study from Oxford Clinical Infectious Diseases found that "single-use medical masks are preferable to cloth masks, for which there is no evidence of protection and which might facilitate transmission of pathogens when used repeatedly without adequate sterilization."
Hmm. Sitting in a cloth mask all day without sterilization could transmit pathogens (organisms that can transmit diseases). Interesting.
● Danish randomized controlled trial with 6,000 participants, published in the Annals of Internal Medicine in November 2020, found no statistically significant effect of high-quality medical face masks against SARS-CoV-2 infection in a community setting.
Other countries get it. We, apparently, don't.
Even UNICEF, which is pro-mask in general (and, I would add, seems to not be following the science by recommending cotton masks), strongly advises against kids under age 5 wearing masks, and recommends mask-wearing for children ages 6-11 only in certain settings.
This is in direct opposition to airlines and some city governments mandating masks for children as young as age 2.
The UK removed face mask requirements for students in May. Education secretary Gavin Williamson said, "Removing face masks will hugely improve interactions between teachers and students, while all other school safety measures will remain in place to help keep the virus out of classrooms."
A Swedish student was kicked out of class for refusing to take off his mask. As noted above, the Netherlands only urges mask wearing for people 13 and over.
Also, keep in mind that mask-wearing has been a prevalent trend in Asia — China, specifically — for years, and that obviously didn't stop the virus from originating and spreading there.
And maybe it's also worth noting that many of the same people mandating/advocating for these rules aren't always following them (like Lori Lightfoot, Gretchen Whitmer, Gavin Newsom, Barack Obama, Muriel Bowser and Nancy Pelosi, to name a few). Just something to consider.
Even if masks were proven to be super effective, kids have a very, very, very small chance of getting anything close to a severe case of COVID.
The American Academy of Pediatrics finds that pediatric hospitalization of kids because of COVID is extremely rare. A recent study found that some hospitals are reporting children admitted to the hospital with COVID symptoms, or who tested positive for COVID, but who were not admitted because of COVID:
Children have suffered tremendously due to policies that have kept schools and recreational facilities closed to them, and the burden has been greatest on children who are low-income and English language learners. Scientific and media reports that inaccurately portray the risk of COVID-19 to children can do harm by alarming parents and providing justification for ongoing restrictions to in-person education and other programming (i.e. summer camps). Kushner et al and Webb et al have contributed greatly to the field by careful work to understand the true burden of COVID-19 disease among children. Via these studies, parents and policy makers should be reassured that pediatric hospitalization for severe COVID-19 disease is indeed rare.
Dr. Roshni Mathew, a Stanford School of Medicine pediatric infectious disease specialist, told NPR: "For children in particular, the risk of serious consequences from COVID-19 is the same magnitude as the risk they face from the flu, she says. But many parents seem more worried about the new and less familiar disease. That anxiety is heightened by the new guidelines on mask-wearing. But experts urge parents to try not to worry too much."
If we're to take the CDC's numbers at face value (there may be a reason or two not to), 416 children have reportedly died "with COVID" out of 74 million children in the U.S. Most, it seems, had underlying conditions. These facts, taken with the AAP's warning we previously noted about inflated pediatric hospitalization numbers, lets us know that there is almost a 0% chance of healthy kids dying from the virus.
While every life lost matters, it's important to have some perspective.
In the 2017-18 flu season, the CDC estimates that 643 children 17 and under died of the flu.
Deaths in children with laboratory-confirmed influenza virus infection are reportable in the United States and 183 deaths were reported for the 2017-2018 season. However, influenza-associated pediatric deaths are likely under-reported as not all children whose death was related to an influenza virus infection may have been tested for influenza. Therefore, we used a mathematical model to estimate the total number of pediatric deaths based on hospitalization rates and the frequency of death in and out of the hospital from death certificates, estimating that there were more than 640 deaths associated with influenza in children.
Keep in mind, too, that flu seasons are about six months. We've had COVID for over a-year-and-a-half. So, far more children died of/with the flu in six months a few years ago than have died of/with COVID in the last 18+ months. There were 11 million kids who tested positive for the flu in the 2017-18 season. There have been 4 million children who have tested positive for COVID so far.
Did anyone suggest shutting down schools or wearing masks in 2018? Why not? Because, until COVID, we understood the importance of kids receiving in-person instruction unencumbered by plexiglass and pathogen-laden face cloths. The only thing that's changed, at least for this age group, is politics. As Matt Walsh said in a school board meeting recently, the masks are really more about security for the teachers, school board and administration, not for the kids.
Even if kids do get it, they're unlikely to pass to teachers (who, by the way, can get vaccinated if they want to).
Studies in Sweden, France, Wales, and China show that transmission from a child to an adult, mask or not, is extremely rare. From the University of Vermont:
"The data are striking," said Dr. Raszka. "The key takeaway is that children are not driving the pandemic. After six months, we have a wealth of accumulating data showing that children are less likely to become infected and seem less infectious; it is congregating adults who aren't following safety protocols who are responsible for driving the upward curve."
The risk of mask-wearing for kids simply outweigh the benefits.
Dr. Marty Makary, professor at the Johns Hopkins Bloomberg School of Public Health, wrote this about the adverse effect of masks on kids for the Wall Street Journal:
In March, Ireland's Department of Health announced that it won't require masks in schools because they "may exacerbate anxiety or breathing difficulties for some students." Some children compensate for such difficulties by breathing through their mouths. Chronic and prolonged mouth breathing can alter facial development. It is well-documented that children who mouth-breathe because adenoids block their nasal airways can develop a mouth deformity and elongated face.
The possible psychological harm of widespread masking is an even greater worry. Facial expressions are integral to human connection, particularly for young children, who are only learning how to signal fear, confusion and happiness. Covering a child's face mutes these nonverbal forms of communication and can result in robotic and emotionless interactions, anxiety and depression. Seeing people speak is a building block of phonetic development. It is especially important for children with disabilities such as hearing impairment.
In summary…
Kids are at extremely low risk of severe COVID illness. They are not driving the spread of COVID to adults. Plus, everyone 12 and over has had the opportunity to get vaccinated. If the vaccines work, everyone who has taken it is protected, and everyone who has chosen not to take the vaccine has accepted whatever risks that choice may or may not pose. There is therefore no reason to treat kids as if they are a threat to public health.
Furthermore, there is no solid evidence to prove that masking kids is an effective strategy in mitigating COVID, and, in fact, there is plenty of evidence to the contrary. Parents can protect their kids as they see fit, but they should not be forced to wear masks. Follow the science.