Manjurul/Getty Images
Is there anything produced or approved by our government for COVID that isn't ineffective, doesn't have terrible side effects, and doesn't actually make the virus worse? The lockdowns, masks, and shots not only failed to work, but caused terrible collateral damage, failed to stop the virus, and, in fact, likely made the virus become more virulent. Now there are reports that remdesivir, which we already know doesn't work and causes renal and liver failure, might also be making the virus itself worse.
Antiviral agents, whether vaccine or therapeutic, must be perfect. If they fail to fully work, they can create viral immune escape, whereby the virus learns how to mutate around them. It's sort of like the principle of shooting at the king and missing, a principle we are often concerned with regarding the overuse or misuse of antibiotics.
Researchers from the Yale School of Medicine posted a preprint study in which they discovered a mutated version of SARS-CoV-2 that appears to have redeveloped in a previously infected immunocompromised woman who was treated with remdesivir. Researchers were able to sequence the genome in a way that made it clear it was related to the remdesivir use in the patient. The patient was later cured by monoclonal antibodies. "This case illustrates the importance of monitoring for remdesivir resistance and the potential benefit of combinatorial therapies in immunocompromised patients with SARS-CoV-2 infection," the study's authors wrote.
Obviously, this mutation appears to be a rare find, but why would we run the risk of spending $3,000 a person on a therapeutic that doesn't work anyway if it may create immune escape?
Which raises the question: Why are we not treating everyone early with therapeutics like Regeneron, ivermectin, hydroxychloroquine, and other proven safe, cheap, and effective drugs that don't case renal failure like remdesivir and don't run the risk of inducing mutations? This is particularly important for those who are immunocompromised. The last thing people who already have fragile organs should be taking is remdesivir.
In many respects the fact that remdesivir was ever approved and is still the only standard of care, as it kills patients and lines the pockets of both hospitals and the maker, Gilead, is possibly the worst scandal of this entire ordeal. On Feb. 5, Reuters reported that none other than the Wuhan Institute of Virology of the China Academy of Sciences sought a patent on Gilead's remdesivir, a failed drug repurposed from treatment of Ebola, based on the alleged improvement of a single individual COVID patient reported in the New England Journal of Medicine. Incidentally, the only drug ever approved for COVID was developed by Dr. Ralph Baric's lab at UNC Chapel Hill, the same lab that applied for the coronavirus spike protein gain-of-function research and is suspected by many to be behind the creation of this virus.
Gee, is it surprising that the drug developed and pushed early by the same two labs likely behind the virus is not only a dud but dangerous?
But it gets worse. On Dec. 12, 2019, less than five months before Fauci and the FDA pushed approval of remdesivir without consulting with an outside panel of experts, the New England Journal of Medicine published a study on remdesivir use in Ebola that should have gotten the drug permanently banned for any use. Over the preceding year, the researchers conducted a randomized controlled trial of four therapeutics for use against Ebola in the Democratic Republic of Congo: remdesivir and three types of monoclonal antibodies, including Regeneron. What were the results in Table 2 of the study?
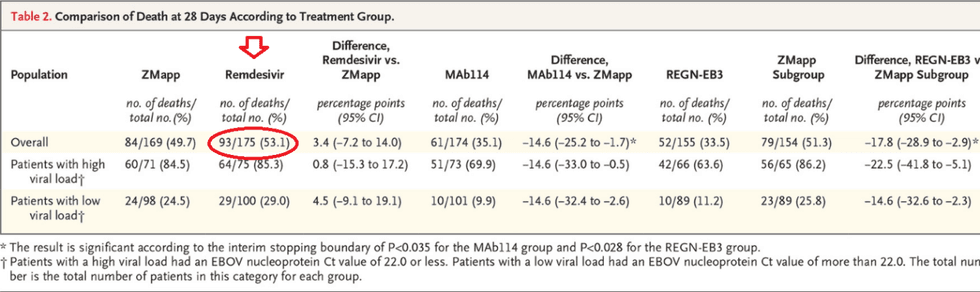
Of the four drugs, remdesivir had the worst outcome with a 53.1% death rate, which is higher than the death rate from the virus. In fact, both remdesivir and ZMapp (death rate of 49.7%) were deemed to be so dangerous that they were pulled from the study on Aug. 9, 2019. Incidentally, Regeneron, which had the lowest death rate, is the monoclonal antibody therapy that seems to work well for COVID. Why would Fauci first pick remdesivir over Regeneron?
On April 29, Fauci announced that remdesivir would become the standard of care, and another study he cited was Gilead's own March 2020 study (eventually published in the NEJM in June) of 53 coronavirus patients in the U.S. Canada, Europe, and Japan who used remdesivir for 10 days. Sixty percent reported adverse events and 23% reported serious adverse events, the most common being "multiple-organ-dysfunction syndrome, septic shock, acute kidney injury, and hypotension." Furthermore, "Four patients (8%) discontinued remdesivir treatment prematurely: one because of worsening of preexisting renal failure, one because of multiple organ failure, and two because of elevated aminotransferases, including one patient with a maculopapular rash."
This is why the NIH to this day warns about renal failure and liver toxicity from the use of this drug that is bankrupting us and killing people in the hospitals. The WHO recommends against using it. The WHO's Solidarity trial, which was conducted on 2,750 patients in 405 hospitals across 30 countries, found "little or no effect of remdesivir on mortality," even though "the proportion of lower-risk patients happened to be appreciably greater in the remdesivir group than in the placebo group."
Last year, in France's Bichat-Claude Bernard University Hospital, researchers studied outcomes in the first five COVID ICU patients who were administered remdesivir. Researchers observed, "Remdesivir was interrupted before the initially planned duration in four patients, two because of alanine aminotransferase elevations (3 to 5 normal range) and two because of renal failure requiring renal replacement." Elevated alanine aminotransferase is usually an indication of liver toxicity, one of the warnings the NIH has given about the use of remdesivir.
To control for the confounding factor that perhaps the kidney failure associated with remdesivir is in fact a symptom of the virus, researchers at the Department of Nephrology-Dialysis-Transplantation at Centre Hospitalier Universitaire de Nice, France, compared the reported incidence of renal failure in COVID patients using remdesivir to those using other drugs. A search of the international pharmacovigilance postmarketing databases (VigiBase) of the World Health Organization (WHO) showed that the reporting odds ratio of acute renal failure for COVID patients on remdesivir "was 20-fold" that of patients treated with hydroxychloroquine, tocilizumab, and lopinavir/ritonavir.
Well over a year after it has become abundantly clear that this drug only causes harm and does not save a single life, not a single hospital has stopped using it. These same hospitals are firing talented doctors either for not getting the failed shots or for using ivermectin. They will even go to court to prevent a dying patient with no other options from being administered ivermectin by an outside doctor. Yet they will use remdesivir to the gates of hell.
For those who simply cannot believe all of the safety concerns and signals about the vaccines, just remember that what we already know from existing data and see right in front of our eyes with remdesivir is perhaps even more scandalous that what is being alleged about the vaccines.